
Wegener’s Granulomatosis (WG), also known as granulomatosis with polyangiitis, is a complex vasculitic condition with diverse systemic manifestations. Often characterized by pauci-immune vasculitis affecting small to medium-sized vessels, WG’s clinical spectrum can be broad and challenging to diagnose. In this case report, we delve into a unique presentation of WG in a 72-year-old female, shedding light on the complexities and diagnostic nuances encountered in her clinical journey.
Also Read: Toy Story Inspiration Jeffrey’s Toys Closes After 86 Years, Blaming San Francisco’s Crime Crisis
Case Presentation
A 72-year-old woman with a history of well-managed type 2 diabetes mellitus and hypertension presented to the hospital with recurrent nasal congestion, headaches, and intermittent facial pain over a two-month period. Initially diagnosed with pansinusitis, her condition took an unexpected turn with the development of bilateral lower limb numbness and weakness. Serial investigations eventually led to a WG diagnosis, highlighting the importance of considering vasculitic conditions even when autoantibody tests yield inconclusive results.
Clinical Manifestations and Diagnostic Challenges
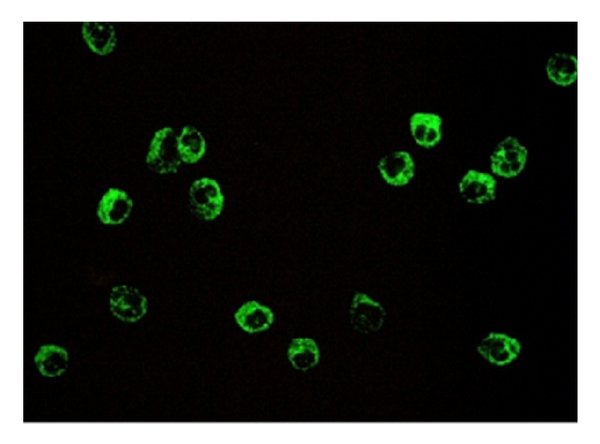
WG’s granulomatous inflammation can manifest across multiple organ systems, with neurological involvement occurring in a significant percentage of cases. The presence of antineutrophil cytoplasmic antibodies (ANCA), specifically perinuclear (p)-ANCA positivity, remains a rare finding. The case emphasizes the need for a comprehensive diagnostic approach, considering the diverse clinical presentations that may not align with typical autoantibody patterns.
| Investigation | Initial Value | 2 Weeks After | Reference Range | |
| Full blood count | White cell count (× 103/µL) | 15.3 | 10.66 | 4–11 |
| Neutrophils (× 103/µL) | 12.09 | 7.79 | 1.5–7.5 | |
| Hemoglobin (g/dL) | 10.7 | 7.9 | 12–14 | |
| Mean corpuscular volume (fL) | – | 88 | 80–100 | |
| Mean corpuscular hemoglobin (pg) | – | 28.85 | 27–32 | |
| Platelets (× 103/µL) | 386 | 184 | 150–400 | |
| Inflammatory markers | CRP (mg/L) | 177 | 5 | <5 |
| Erythrocyte sedimentation rate (ESR) (mm in the first hour) | – | 110 | <20 | |
| Renal profile | Serum creatinine (µmol/L) | 94 | 366 | 53–97.2 |
| Serum sodium (mmol/L) | 129 | – | 135–145 | |
| Urine full report | Pus cells (per high-power field) | 3–5 | 2–4 | |
| Red cells (per high-power field) | 10–12 | Moderately field full | ||
| Red cell casts | Negative | – | ||
| Imaging studies | Ultrasound scan of the abdomen | Grade 1 fatty liver | Normal renal morphology | |
Discussion: Understanding Wegener’s Granulomatosis
Formerly known as Wegener’s granulomatosis, GPA is an ANCA-associated small vessel vasculitis characterized by necrosis, granulomatous inflammation, and vasculitis. C-ANCA, directed against proteinase 3, is a hallmark, but its absence does not rule out the diagnosis. The disease predominantly affects the upper and lower respiratory tracts and kidneys, leading to a varied clinical presentation, including ocular, gastrointestinal, cardiac, skin, and nervous system manifestations.
Diagnostic Dilemmas and Multidisciplinary Management
The case presented challenges in diagnosis, with inconclusive initial investigations. GPA’s classification criteria and disease states were explored, and the patient’s severe and active disease state guided the choice of treatment. A multidisciplinary approach involving nephrology, pathology, and neurology was crucial for effective management.
Treatment Strategies: Striving for Remission
Early initiation of remission induction is paramount in preventing organ damage. Corticosteroids are foundational, with rituximab or cyclophosphamide recommended for severe cases. Rituximab, preferred for its lower toxicity, demonstrates efficacy in achieving remission. Nonsevere GPA is managed with methotrexate for remission induction, while remission maintenance involves rituximab, methotrexate, azathioprine, or mycophenolate mofetil.
Conclusion: Navigating Wegener’s Granulomatosis
Timely identification and comprehensive treatment are imperative in managing Wegener’s granulomatosis. Despite diagnostic challenges, this case underscores the significance of a multidisciplinary approach and the effectiveness of rituximab in achieving remission. Understanding the varied clinical presentations and treatment nuances is crucial for optimizing outcomes in Wegener’s granulomatosis.
Also Read: Steve Smith Faces Criticism Over Dropped Catches and Batting Struggles Against West Indies

Pingback: American Airlines Hard Landing in Maui: FAA Investigates as Passengers and Crew Endure Minor Injuries - 𝐋𝐈𝐎𝐍𝐉𝐄𝐊 News